7th World Bronchiectasis and NTM Conference
The 7th World Bronchiectasis and NTM Conference provides education around epidemiology, pathogenesis, diagnosis, management and treatment of bronchiectasis and nontuberculous mycobacteria (NTM).






Chronic cough

Dyspnoea
Daily sputum production
Fatigue
Recurrent infections

Haemoptysis
Data from a study of 2,572 patients with bronchiectasis from 10 clinical centres across Europe and Israel showed that:13
Patients with 2 or more exacerbations per year at baseline had a 60% increased risk of 5-year all-cause mortality.
Patients with 3 or more exacerbations per year at baseline had an 86% increased risk of 5-year all-cause mortality.
Cough
Fatigue and/or malaise
Breathlessness and/or exercise intolerance
Haemoptysis
Sputum volume and/or consistency
Sputum purulence
Preventing exacerbations can help make a positive impact on patients both physically and mentally.7,13
It’s important that patients are educated about the consequences of exacerbations and the appropriate actions to take, including when to seek medical help and report them to their treating physician.
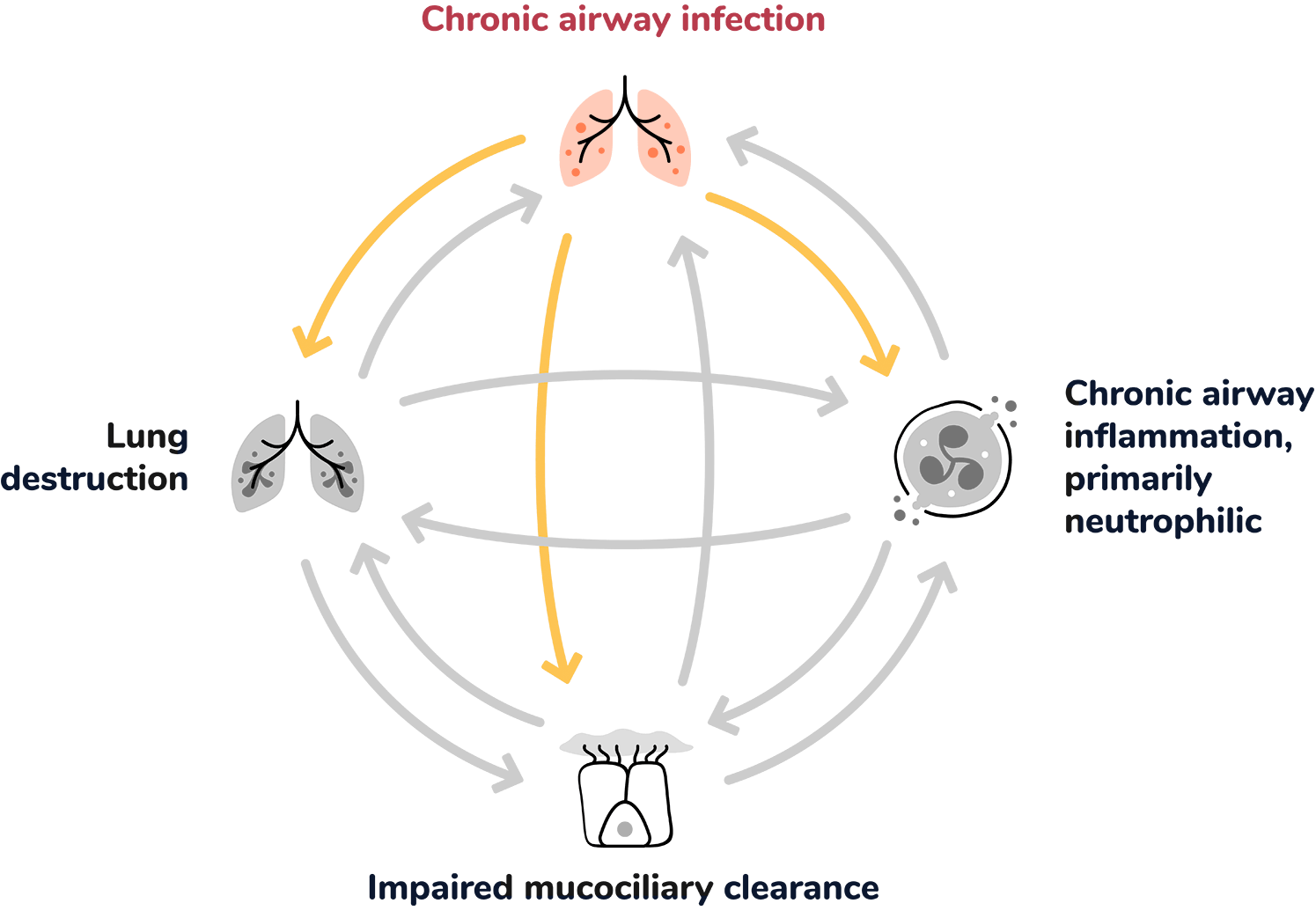
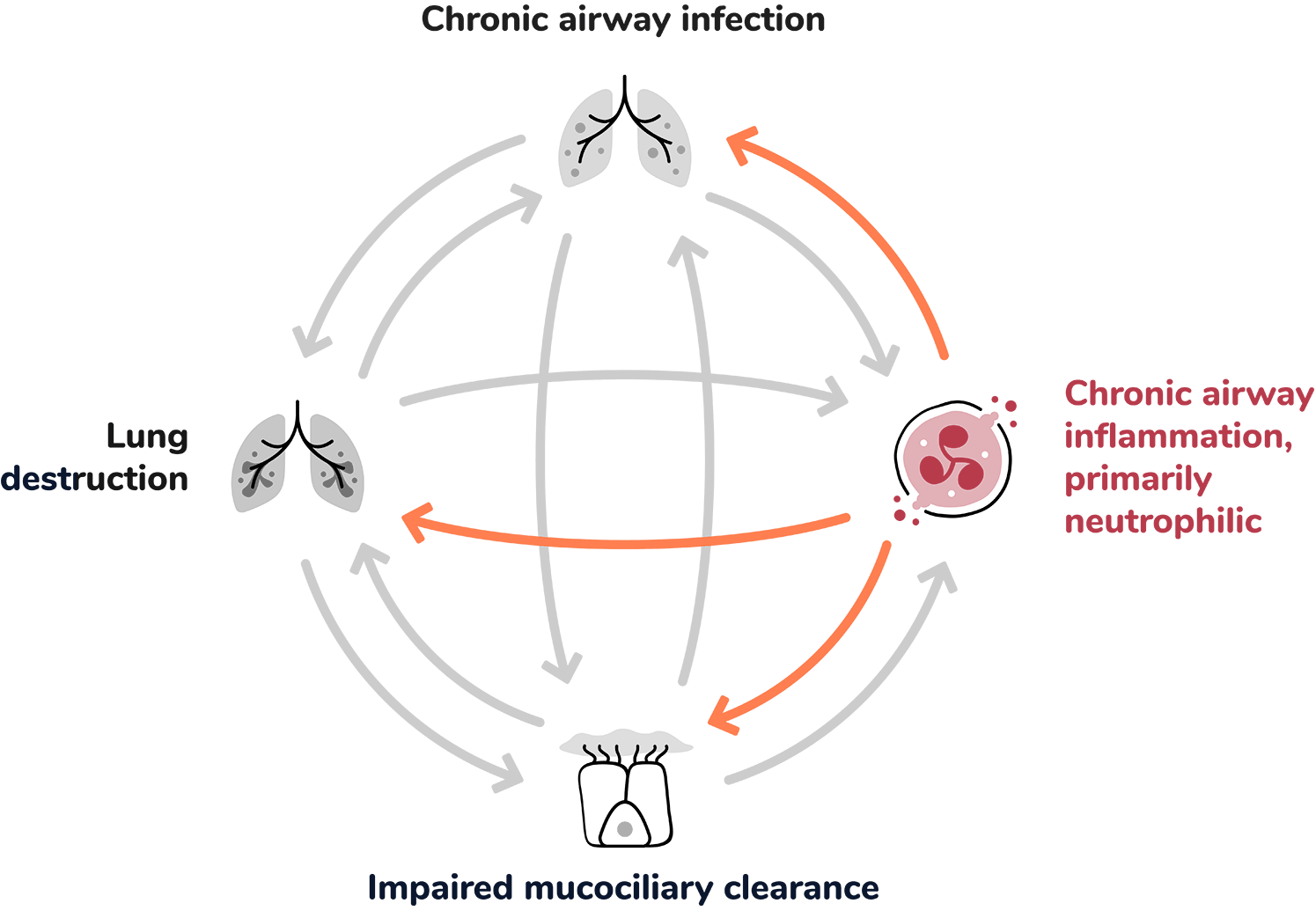
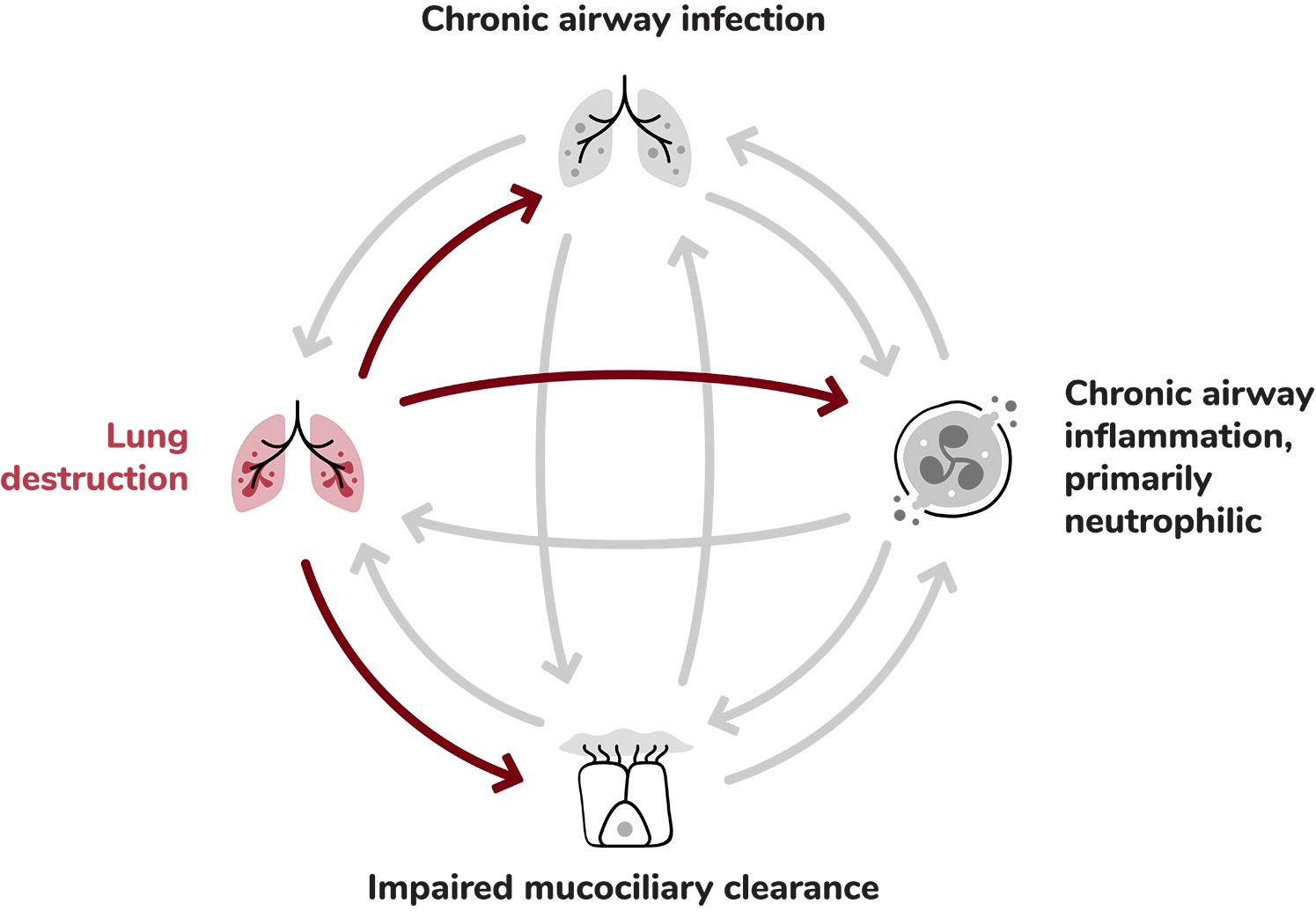
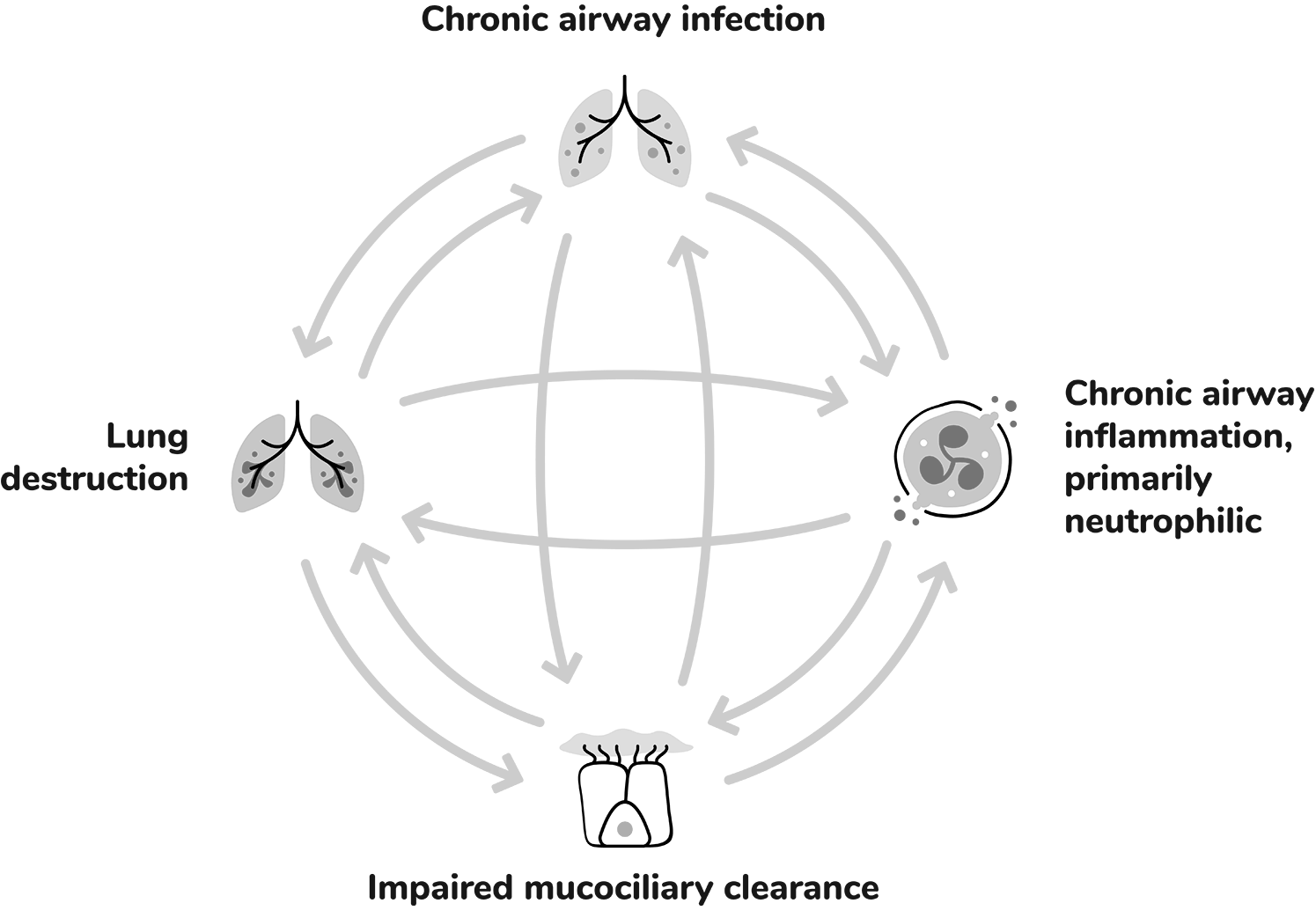
Within the self-perpetuating cycle of bronchiectasis, each driver can lead to the worsening of the others and contribute to progressive lung damage and exacerbations.1,5
Chronic airway infection contributes to the pathophysiology of bronchiectasis by inducing chronic airway inflammation, which can lead to progressive airway damage and injury.1
Extensive infiltration of the airways by inflammatory cells: 1,5,7
Dysfunctional mucociliary clearance can lead to sputum retention in airways, creating a harbour for infection and inflammation.1
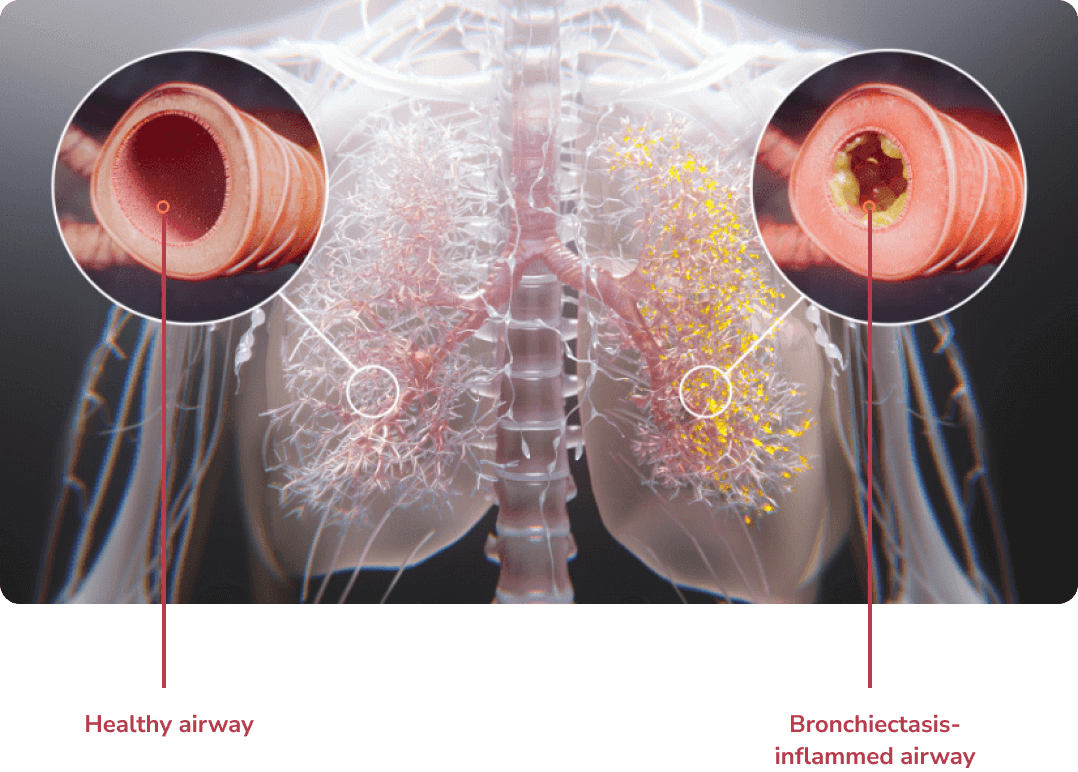
Structural lung damage involving bronchial wall destruction and dilation.1
Click to explore
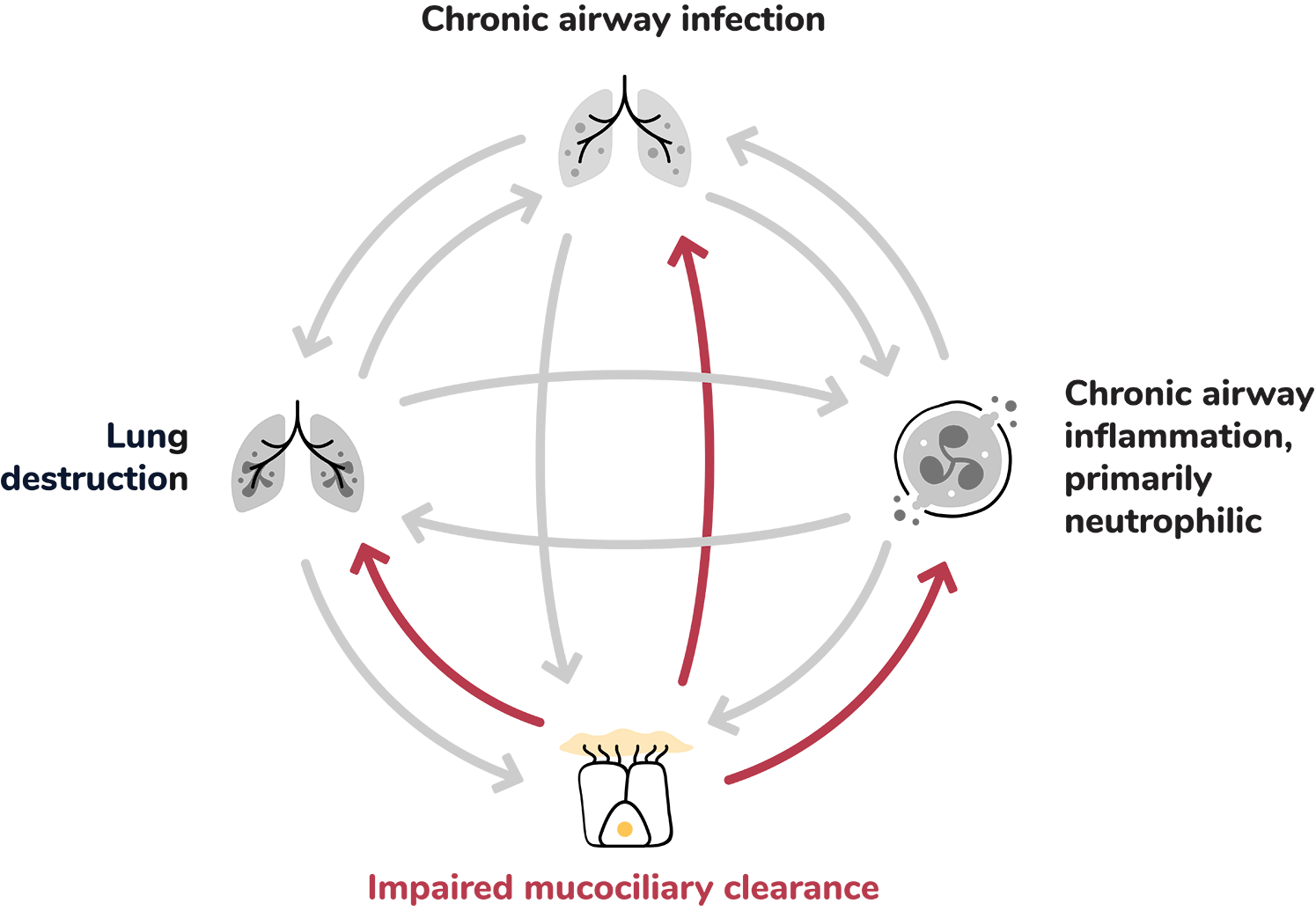
Chronic airway infection contributes to the pathophysiology of bronchiectasis by inducing chronic airway inflammation, which can lead to progressive airway damage and injury.1
Extensive infiltration of the airways by inflammatory cells: 1,5,7
Dysfunctional mucociliary clearance can lead to sputum retention in airways, creating a harbour for infection and inflammation.1
Structural lung damage involving bronchial wall destruction and dilation.1
Register to receive updates and information about bronchiectasis.
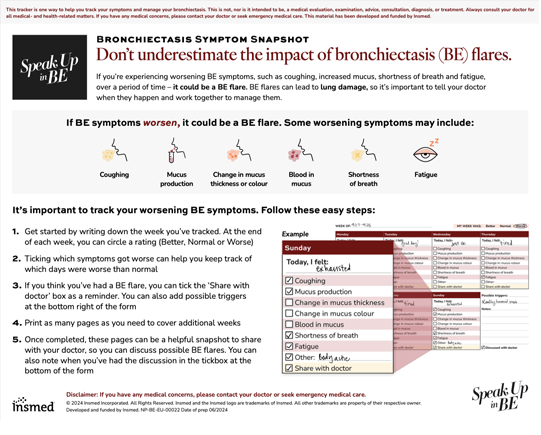
Patients can use this tool to help keep track of BE symptoms and possible BE exacerbations between appointments.
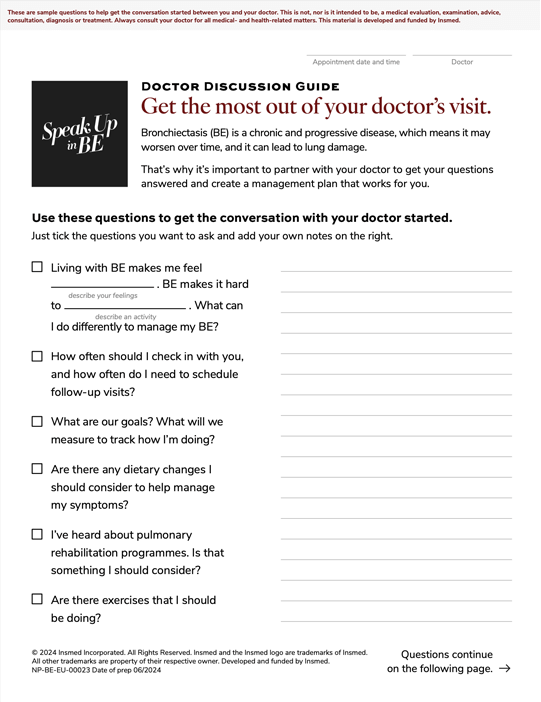
Patients can use these important questions about BE as a guide to support their next doctor’s appointment.

7th World Bronchiectasis and NTM Conference
The 7th World Bronchiectasis and NTM Conference provides education around epidemiology, pathogenesis, diagnosis, management and treatment of bronchiectasis and nontuberculous mycobacteria (NTM).
4–6 July 2024
Dundee, Scotland

European Respiratory Society Congress 2024
The European Respiratory Society Congress is an annual event that brings together the world’s respiratory experts to showcase all the latest advances in respiratory medicine and science.
Visit Insmed at booth C7.03 Hall B
7–11 September, 2024
Vienna, Austria